Where we stand with the COVID-19 pandemic and case-based solutions
Trevor Bedford (@trvrb)
Associate Professor
Fred Hutch, Seattle, WA
28 Apr 2020
Talk overview
- How we got here
- Where we are now
- How we get out here
How we got here:
Genomic overview of the COVID-19 pandemic, using viral sequencing to reconstruct
SARS-CoV-2 evolution and spread
Epidemic process

Sample some individuals

Sequence and determine phylogeny

Sequence and determine phylogeny

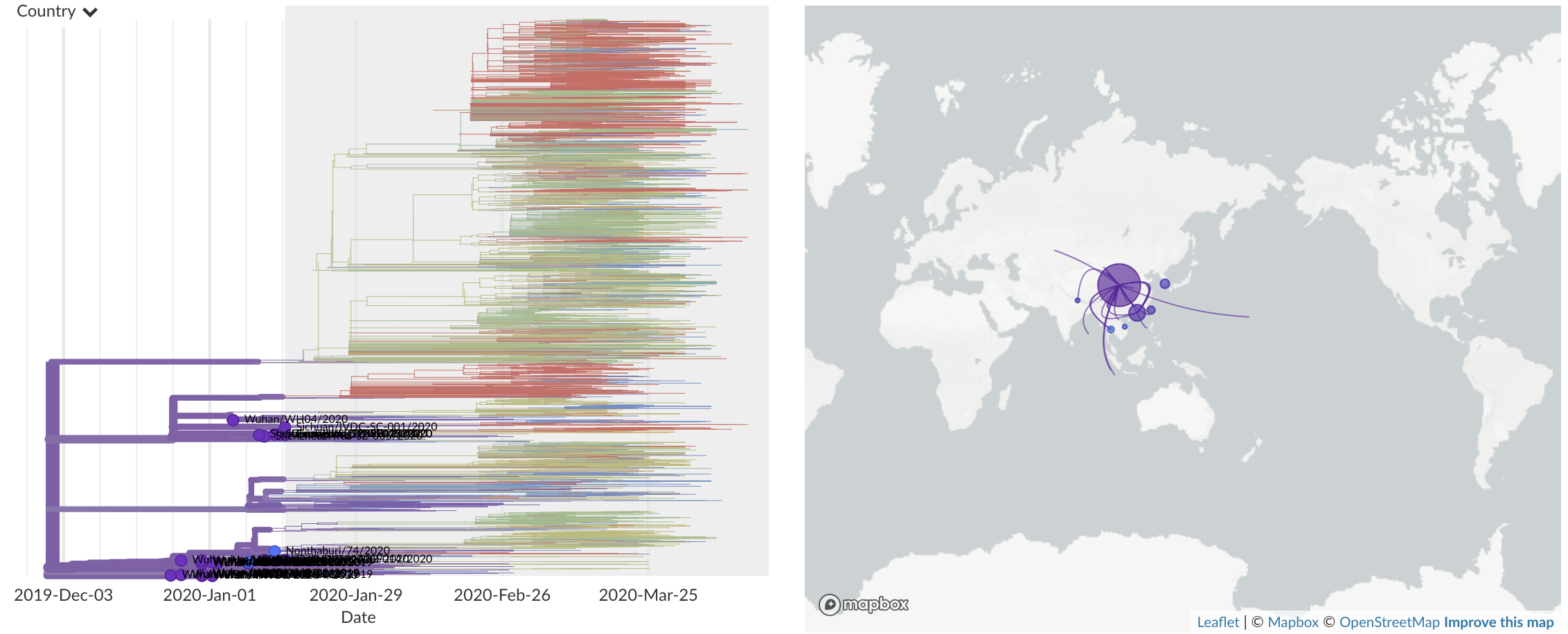
Dec/Jan: Emergence of SARS-CoV-2 from Wuhan in ~Nov 2019
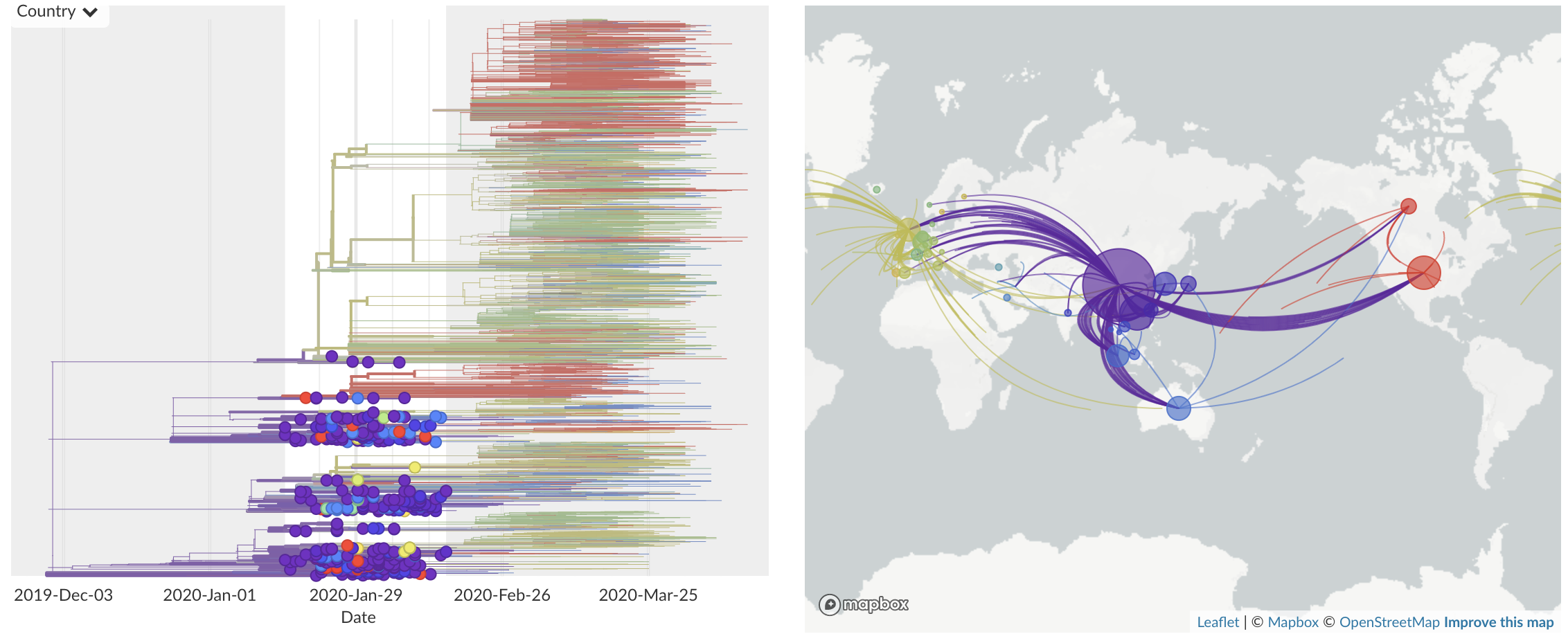
Jan/Feb: Spread within China and seeding elsewhere
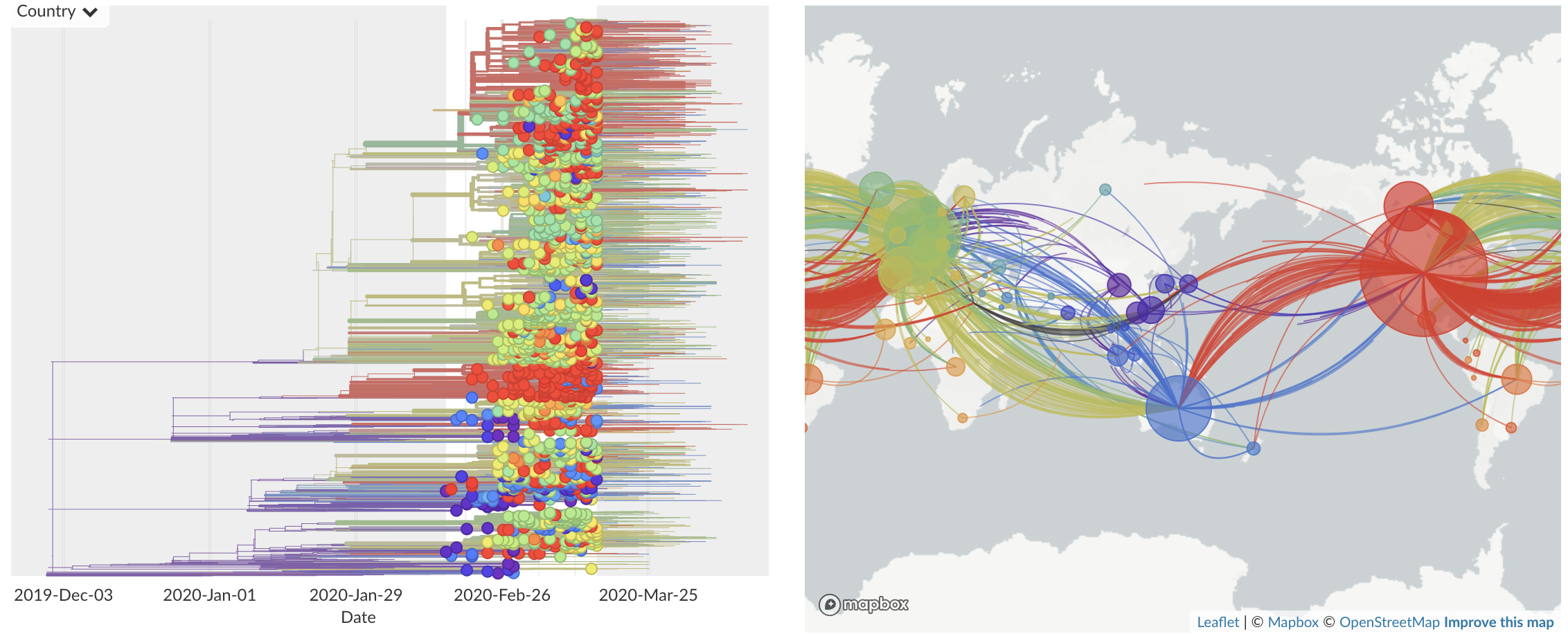
Feb/Mar: Epidemic spread within North America and Europe
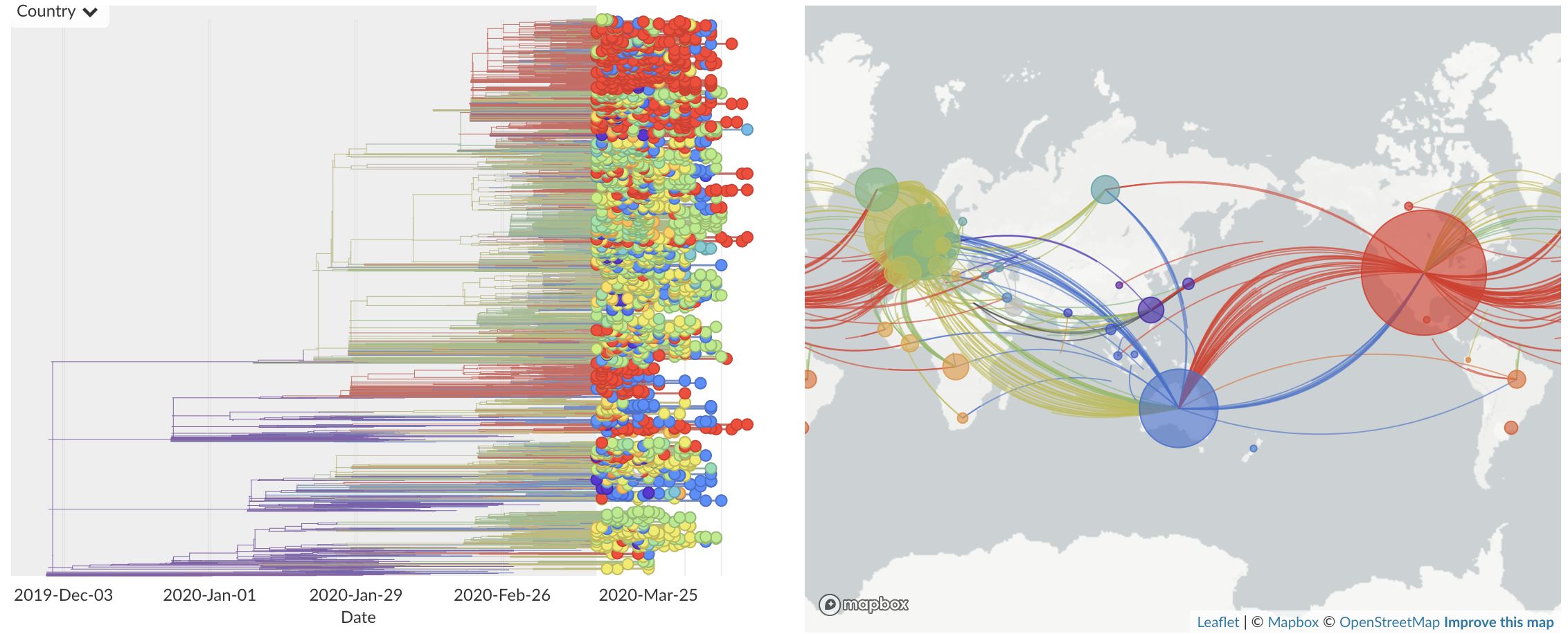
Mar/Apr: Continued growth, but decreasing transmission with social distancing measures
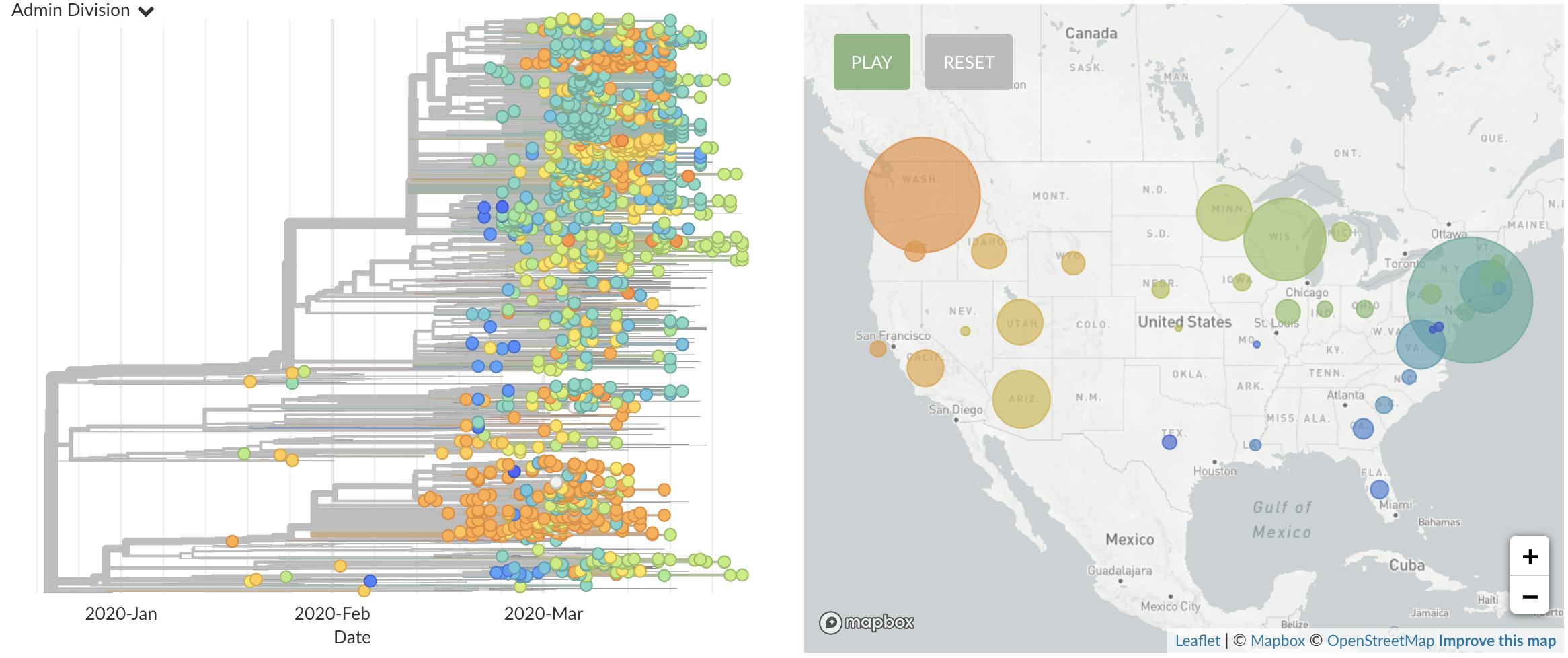
Epidemic in the USA was introduced from China in late Jan and from Europe during Feb

Once in the US, virus spread rapidly
Where we are now:
Plateau of detected cases, but continued transmission
With social distancing we've seen substantial drops in transmission, but not suppression

Transmission is heterogeneous across the US

My numbers
- Current plateau at ~30,000 cases reported per day with ~1M total confirmed cases reported
- With 10-15X underreporting, this is likely 300k to 450k infections per day and between 10M and 15M total infections
- NYC may have 30% seropositivity at this point, I'd guess ~3-5% nationally
- Herd immunity likely requires at least 66% recovered
- Infection-to-fatality ratio in general population of 0.5% to 1.0%, much of which has yet to be realized in the currently ill
How we get out of here:
Case-based interventions to mitigate spread
Moving forward
- Suppression has failed
- Facing a long period of localized flare-ups and societal responses
- Recommend strategies to mitigate spread while keeping economy functioning
- Scalable case-based interventions (testing, contact tracing and isolation)
- Non-disruptive distancing and hygiene
Fundamental importance of contact tracing and quarantine of exposed contacts
This is due to the large fraction of presymptomatic (and perhaps asymptomatic) transmission. Contact tracing of symptomatic index cases more efficient and efficacious than biweekly population testing (Kucharski et al). Requires speed (exposures alerted within 48 hours from index case developing symptoms) and scale (currently ~300k infections per day).
Example transmission chain and intervention

Example transmission chain and intervention

Requirements for contact tracing at scale
- Scale up of testing. We need to be testing to be readily available for mild cases and free to access. Testing mild cases helps adherence to isolation. Testing early in the course of illness is most beneficial.
- Workforce development. Models based on current workflows estimate 180k people to support tracing 30k daily confirmed cases and follow up with their contacts.
- Wrap around services. Voluntary self-isolation facilities. Income support for self-isolation.
- Digital tools to increase efficiency and efficacy of case investigation and organize efforts (possibly involving privacy-preserving proximity apps).
Reducing transmission rate reduces final epidemic size

Reduction in transmission pays dividends
- Confirming 1 case in 5 and successfully quarantining 50% of their contacts would reduce $R_0$ by 10%
- $R_0$ of 1.5 (achieved through hygiene and social distancing) translates to 191M eventual infections
- $R_0$ of 1.35 (with the addition of scalable contact tracing) translates to 154M eventual infections
- This is roughly 18M averted symptomatic infections (assuming a 50% symptomatic rate), 180k averted deaths (assuming IFR of 0.5%) and $56B in averted direct medical costs
Acknowledgements
Genomic epi: Data producers from all over the world, GISAID, Virological.org and the Nextstrain team